

Abstract
Islet transplantation has been shown to be a viable treatment option for patients afflicted with type 1 diabetes. However, the lack of availablity of human pancreases and the need to use risky immunosuppressive drugs to prevent transplant rejection remain two major obstacles to the routine use of islet transplantation in diabetic patients. Successful development of a bioartificial pancreas using the approach of microencapsulation with perm-selective coating of islets in hydrogels for graft immunoisolation holds tremendous promise for diabetic patients because it has great potential to overcome these two barriers. In this review article, we will discuss the need for a bioartificial pancreas, provide a detailed description of the microencapsulation process, and review the status of the technology in clinical development. We will also critically review the various factors that will need to be taken into consideration in order to achieve the ultimate goal of routine clinical application.
Introduction
Polyuria, polydipsia, polyphagia, weight loss and fatigue are early symptoms of diabetes mellitus, a common disorder of glucose homeostasis marked by a deficiency or lack of a small polypeptide known as insulin. Before the discovery of insulin, patients suffering from diabetes literally starved to death, their tissues awash in glucose, but with the cells lacking the ability to admit this simple sugar. In the late 1880s, von Mering and Minkowski observed that pancreatectomized dogs developed glycosuria, implicating the pancreas in the disorder causing diabetes, and subsequently, Opie and others identified pathological changes in the islets of Langerhans by histological study of pancreatic tissue taken from patients with diabetes [1]. Nearly 90 years ago, Banting, Best, Colip and Macleod won the race to discover the pancreatic ‘principle' largely responsible for glucose homeostasis, and Banting and Macleod shared the Nobel Prize for this discovery with their colleagues [1].
Prior to the discovery of insulin by Banting and Best, effective treatment of diabetes mellitus was limited to dietary manipulation. The discovery of insulin converted an often rapidly fatal disease (particularly for patients with the clinical equivalent of type 1 diabetes) to a chronic condition requiring life-long treatment. At the time, many thought that the ability to administer insulin exogenously would prove to cure diabetes, but the long-term imperfections in glycemic control present even with state-of-the-art insulin management results in the so-called secondary complications of diabetes, which can significantly diminish the life expectancy and quality of life of many patients [2]. The current treatment for diabetes, both type 1 and type 2, includes exogenous insulin administration and endocrine replacement by solid organ or islet allotransplantation. Both insulin administration and pancreas transplantation have considerable inherent drawbacks, driving the clinical need for new approaches such as the bioartificial pancreas [2].
Therapeutic Options for Type 1 Diabetes
Exogenous Insulin Therapy
Exogenous insulin administration to control blood glucose has been the standard therapy since the discovery of insulin. In this therapy, the amount of carbohydrates consumed is estimated by measuring food, and this is used to determine the amount of insulin necessary to cover the meal. The calculation is based on a simple open-loop model based on past success. Calculated insulin is then adjusted based on premeal blood glucose measurement, such that insulin bolus is increased for high blood glucose or decreased for low blood glucose. Insulin is injected or infused subcutaneously and enters the blood stream in approximately 15 min. Blood glucose can then be tested again and adjusted by additional insulin bolus or eating more carbohydrates, until a balance is achieved. Needless to say, this procedure leads to rapid blood glucose fluctuations and is highly inefficient both in terms of patient convenience and health. While it has been useful, insulin treatment can also has a negative impact on personal and social functioning. The poor control of blood glucose fluctuations with this therapy leads to many severe secondary complications such as retinopathy, neuropathy, nephropathy and cardiovascular diseases [2,3]. According to the Diabetes Control and Complications Trial (DCCT), strict control of blood glucose may delay the onset of new diabetes-related complications and the progression of existing ones, but would not ultimately prevent the development of secondary diseases associated with diabetes [4].
Pancreas Transplantation
Kelly et al. [5] performed the first clinical pancreas transplant at the University of Minnesota in 1966. Currently, pancreas transplantation is the only option therapeutically available that reproducibly achieves normoglycemia. Pancreas transplantation re-establishes endogenous insulin secretion that is responsive to normal feedback regulation. Since 1966, more than 30,000 pancreas transplants have been performed worldwide. According to the Scientific Registry of Transplant Recipients, the 1-year rate of graft survival is 86% when a pancreas and a kidney are transplanted together, 82% when a pancreas is transplanted after a kidney and 75% when only a pancreas is transplanted. Most pancreatic grafts are from cadaveric donors, though transplantation of a segment of the pancreas donated by a living donor has also been reported [6]. Transplantation, however, requires major surgery and dependence on life-long immunosuppression to prevent graft rejection. Most pancreas transplants are performed with immunosuppression induction therapy (usually monoclonal or polyclonal T cell-depleting antibody) and maintenance immunosuppression with a calcineurin inhibitor (cyclosporine or tacrolimus), an antimetabolite (mycophenolic acid) with or without corticosteroids [7,8]. Owing to the limited availability of human pancreases and the need for immunosuppression, relatively few pancreas transplants are performed in relation to the entire diabetic population. Improvements in surgical technique or immunotherapy are also unlikely to make whole-organ pancreas transplantation available to the majority of patients with diabetes.
Islet Transplantation
Islet transplantation promises to be a cure at least as effective as pancreas transplantation, while being much less invasive. The efficiency of islet recovery from the pancreas and the susceptibility of allogeneic islet to immune attack (both alloimmunity and autoimmunity) are the two major barriers to successful islet transplantation. There are approximately 1 million islets in an adult human pancreas. However, only half or fewer of these are successfully isolated on a consistent basis. Thus, islet transplantation usually requires islets isolated from two or more donor pancreases. As islet isolation requires manipulation of human tissue, the process must be carried out in a GMP (good manufacturing process) facility, which adds to the expense of the procedure. Islets are transplanted by transfusion into the portal vein and embolization into the liver. The transplanted islets engraft in the distal portal triad (fig. 1). Allogeneic human islets have been successfully transplanted using the Edmonton immunosuppression (steroid-free) protocol [9]. With this protocol, glycemic control has been restored for extended periods of greater than 5 years in a few patients, but at the expense of the immunosuppression of the transplant recipient. The necessary life-long adherence to an immunosuppression drug regimen is inconvenient and is associated with side effects and the complications of overimmunosuppression.
![Fig. 1. Illustration of islet transplantation ([59] with permission).](https://karger.silverchair-cdn.com/karger/content_public/journal/pat/80/4/10.1159_000345873/2/m_000345873_f01.jpeg?Expires=1716300458&Signature=N~4bJpVUa1itmHXrVBFjWBDKE0lp~NIzoRODUtO~MEHBk0DsDLBEhuijbzfJQNYCmlQIVtuOYYtuLajacYPNq8fZj31JB3qi0KyxXy0m5hF9sYN11-mXbQhT~ctdg0ylC-h5CorIR0Mjyek0Co3FFphIBHYpfj7FbDd2tmc2KoPKVt87dwfx5ywTedJN9vDe1RJxiiSfLUwDnf~H1kgNJMlmejEmvbQ2qE2CTvMsn7OmKS2mQco6Ba-Z5VvddhQG2nDQ59Xw4cilNTqVwbsx62xF0M-SQ2Cms-mL4ynwC-5cOUEe4WLKMlTUSWv4qLmiGaabXdr34RNmSOsXrd6CjA__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Artificial Pancreas
The artificial pancreas is a technological development to enable type 1 diabetic patients to automatically control their blood glucose, acting, in essence, like a healthy pancreas. The goals of the artificial pancreas are: (1) to improve presently popular but inefficient insulin therapy to attain a better glycemic control, thus avoiding the complications arising from blood glucose fluctuations, and (2) to mimic normal stimulation of the liver by the pancreas and to normalize carbohydrate and lipid metabolism. There are various approaches to the artificial pancreas.
- The medical equipment approach: this is basically an insulin pump under closed-loop control utilizing real-time data from a continuous blood glucose sensor.
- The gene therapy approach: this involves therapeutic infection of a diabetic person by a genetically engineered virus causing a DNA transformation of a few intestinal cells to become insulin-producing cells. It has even been suggested as a strategy to tackle the cause of β cell destruction itself, hence curing the patients before full and irreversible β cells destruction occurs [10]. While novel and potentially able to treat diabetes, this approach is still in its infancy with a lot of unanswered questions.
- The bioengineering approach: this attempt to design a bioartificial pancreas has generally involved the development of either microcapsules, or macrocapsules, or of other devices such as a biocompatible sheet of encapsulated islets. When implanted, these constructs would substitute the defective native endocrine pancreas [11]. However, this review focuses on the microencapsulated islet construct, as it has advanced into the stage of clinical trials [12,13,14,15] and holds significant promise for being a good alternative to pancreas transplantation. Using alginate as the encapsulation polymer, the concept of islet immunoisolation (fig. 2) essentially incorporates a semipermeable membrane into the process because alginate does not have any appreciable perm-selectivity towards immune cells and other immunological factors such as antibodies that could potentially destroy the encapsulated cells.
A Bioartificial Pancreas
Materials
Alginate
The chemical structure of alginate consists of unbranched binary copolymers of 1-4-linked β-D-mannuronic acid (M) and α-L-guluronic acid (G), illustrated in figure 3. Both the composition and block structure vary in different types of alginate, but the length of the G blocks is the main structural feature that contributes to gelation because the diaxially linked G residues form cavities that function as binding sites for ions [16]. As already mentioned, alginate gels easily in the presence of divalent cations, such as Ca2+, Sr2+ and Ba2+, which interact with Na+ ions from the G-monomers in the polymer chains to form ionic bridges between adjacent polymers [16,17]. Among the possible cross-linking cations for alginate microbeads, Ba2+ and Ca2+ have been the most researched in cell microencapsulation studies. For most laboratories, Ca2+ is the preferred divalent cation for alginate cross-linking during cell microencapsulation, because in contrast to Ca2+, Ba2+ binds to both the G and M molecules in alginate, leading to a high degree of cross-linking and greater in vivo stability, albeit leaving no room to equip the alginate microbeads with perm-selectively [18]. There is also some concern about possible Ba2+ toxicity to cells as this divalent cation is a strong inhibitor of K+ channels [19], which are critically involved in the stimulus-secretion coupling of insulin secretion [20]. It is also known that organic solutes used routinely in the generation of Ba2+ alginate beads are cytotoxic when released from microcapsules after transplantation and thus have to be replaced by biomolecules such as histidine [19]. One major advantage of using Ca2+ as the cross-linking cation is that an inner alginate core encapsulating islets can be liquefied in order to enhance the diffusion of permissible molecules to and from the microcapsules [21]. The process of liquefaction is pretty delicate and has to be performed with utmost caution in order to avoid capsule breakage caused by high internal colloid-osmotic pressure after the ‘degelling' [19].

It has been shown that the chemical composition of alginate based on the ratio of G to M blocks, the gelling cation, and the purity of alginate have considerable effects on microbead size and morphology [22,23,24] and on the host tissue response [25,26]. For transplantation experiments, the purity of alginate is critical, as it is very well established that host tissue response is significantly reduced or even eliminated when highly purified alginate is used for encapsulation [18,27]. Ultrapure Keltone LV sodium alginate, commercially available as low-viscosity high mannuronic acid and low-viscosity high guluronic acid preparations from Novamatrix, Sandvika, Norway, is routinely used for cell microencapsulation. In our experience, these alginate preparations can be stored frozen at -80°C for many years without any change in their properties.
Semi-Permeable Membrane Fabrication
Effective immunoisolation of cells in alginate microcapsules is primarily achieved by the incorporation of a perm-selective membrane into the encapsulated cell device, and a number of biopolymers including poly-L-lysine (PLL), poly-L-ornithine (PLO) and chitosan-polyvinylpyrrolidone have been used for this purpose [18,25,26]. Of these materials, PLL has been routinely used, but evidence is emerging that the use of PLO may result in better mechanical strength and smaller pore-size exclusion [28] as well as the enhanced stability of microcapsules [29,30]. The preferred molecular weight range for both PLL (Sigma-Aldrich catalogue No. P4957) and PLO (Sigma-Aldrich catalogue No. P5061) for the purpose of perm-selective coating of alginate microbeads is 15-30 kDa. Both PLL and PLO are polycationic polymers that require covering of their surface with a coat of the more biocompatible polyanionic alginate in order to prevent electrostatic interactions with cells and proteins after in vivo implantation. This external alginate coating of microcapsules has traditionally been performed by simple incubation of the PLL- and PLO-coated microcapsules in a low concentration of alginate solution for a short period of time, usually less than 10 min. However, this thin coating with alginate that is not cross-linked is prone to the risk of degradation in long-term experiments. Recent studies have described a new procedure for cross-linking the external alginate coating with Ca2+ [2,31], which should enhance the long-term stability of the external alginate coat.
Microencapsulation of Islets
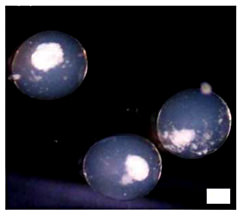
Based on the issues raised above, our laboratory adopts a 4-step process in islet microencapsulation. In the first step, islets are suspended in a solution of sodium alginate (usually from 1.2 to 1.8% w/v) and microspheres of alginate containing one or two islets/microsphere (depending upon the alginate-islet ratio in the suspension), are generated and are allowed to gel into microbeads in a bath of 100 mM CaCl2 solution. Following a couple of washings with normal saline, the microbeads are then perm-selectively coated with variable concentrations of PLL or PLO for a variable duration of time, depending on the desired pore size exclusion limit in the second step. The third step is the liquefaction of the alginate core of the microcapsules achieved by a brief incubation in 55 mM sodium citrate solution. After washings with normal saline again, the final step in the microencapsulation process is the external coating with a lower concentration (routinely about 10% of the concentration used in generating the initial microspheres), but our new procedure utilizes only a slightly lower concentration than the initial alginate concentration used to generate the microspheres [2,31]. To cross-link the external alginate coat, a solution of normal saline supplemented with 22 mM calcium chloride has been recently described for the final washings of microcapsules [31], otherwise normal saline is routinely used. Figure 4 shows some islets encapsulated in alginate-PLO-alginate microcapsules in our laboratory using the 4-step process.
Microencapsulation Devices
The currently available devices for the microencapsulation of islets have been designed based on one of these techniques: (1) interfacial precipitation, (2) phase inversion and (3) polyelectrolyte coacervation. Phase inversion has been mostly used for making macrocapsules, while interfacial precipitation has been applied in the generating of microcapsules. Polyelectrolyte coacervation is a modification of the alginate-calcium interfacial precipitation system, in which complexation of oppositely charged polymers leads to the formation of a hydrogel membrane encapsulating the islets [17]. The two most widely used devices for microencapsulation are the air-syringe pump droplet generator and the electrostatic bead generator [2]. Each of these devices is fitted with a single needle through which droplets of cells suspended in alginate solution are produced and cross-linked into spherical microbeads. A major drawback in the design of these instruments is that they are incapable of producing sufficient numbers of microcapsules in a short period of time to permit mass production of encapsulated and viable cells for transplantation in large animals and humans. It is noteworthy that a prolonged process of encapsulation of cells adversely affects their viability.
A multi-needle approach to producing more than one encapsulated cell at a time as a scale-up of the process has also been described with four needles [32]. While this scale-up is a step forward in accelerating the production of encapsulated cells, production rates at several orders of magnitude higher are required to meaningfully produce sufficient quantities of encapsulated and viable cells to serve millions of patients requiring cell transplantation. For instance, for transplantation in human subjects, it has been estimated that for the 1 million islets needed for transplantation in a diabetic human subject, about 100 h would be required to complete their encapsulation, assuming there would be one islet/microcapsule. In practice, it has actually been estimated that the duration of the process would be closer to 200 h [33] because of the additional steps involved in the encapsulation procedure, following generation of the initial cell-containing alginate microspheres. This situation highlights an urgent need for a radically different approach to rapidly producing viable encapsulated cells in sufficient quantities for routine application in human cell therapy. To address this need, we have recently designed and tested the efficiency of a new scalable prototype device for cell encapsulation using a microfluidic approach [34,35].
Other Critical Factors Affecting the Function of Encapsulated Islets
In addition to the need for effective immunoisolation by incorporating a well-characterized perm-selective membrane in the alginate microcapsule as discussed above, there are other critical factors to be considered when using microcapsules to encapsulate islets for transplantation. We discuss two of these.
Islet Requirements for Oxygen and the Need for Revascularization of Encapsulated Islets
Although islets constitute approximately 1% of the pancreas, they receive about 6-10% of its blood flow [36,37], indicating a disproportionate level of perfusion in which islets receive and consume lots of oxygen. The usual high oxygen requirement of islets is interrupted during the process of islet isolation and processing when they are used for transplantation, and studies have shown that hypoxia has significant deleterious effects on the survival and function of the islets [38]. In the immediate posttransplant period, isolated islets are forced to depend upon diffusion of oxygen and nutrients via peripheral perfusion from the surrounding tissue within the site of transplantation [39] until revascularization by angiogenesis, a process that requires 7-10 days [40]. Routinely, microencapsulated islets are transplanted in the peritoneal cavity, where no revascularization takes place, thus subjecting the islet grafts to extended periods of hypoxia and eventual death. Therefore, as shown in studies performed in large animals and humans, the death of most of the encapsulated islet grafts owing to severe hypoxia results in the need for large quantities of microencapsulated islets to achieve normoglycemia [2].
Regarding the need for oxygen of encapsulated islets, the size of the microcapsule is crucial for their function. The major drawback of macrocapsules is their relative low surface to volume ratio, which interferes with the optimal diffusion of nutrients and oxygen. A small size of microcapsule would benefit the islet and also exponentially decrease the total transplant volume. A significant amount of work has been done with various new technologies to make beads as small as 185 μm (diameter), which is about four times smaller than conventional beads (800 μm). The smaller the diameter of the capsules, the better the diffusion of nutrients to the islets. Omer et al. [41] demonstrated that capsules with a diameter of 600 ± 100 μm showed improved stability in vivo compared to larger capsules with diameters of 1,000 ± 100 μm. In most tissues, it has been shown that the maximum diffusion distance for effective oxygen and nutrient diffusion from blood capillary to cells is 100 μm, which is exceeded when islets with an average diameter of <200 μm are enclosed in conventional microcapsules with average diameters of approximately 800 μm. The absence of this convection inside a capsule induces a nutrient-gradient from the capsule surface to the center of the islet. However, the caveat is that with reduction in capsule size, the number of capsules containing partially protruding islets also proportionally increases, and this in turn increases the number of capsules affected by an inflammatory response. Decreasing the islet density in alginate can solve this problem, as it has been shown that each capsule size has an optimal islet density. Usually, this is associated with a slight increase in empty capsules, but minimizing protruding islets is of utmost priority. In many cases, the inner alginate bead will be either completely or partially liquefied by the removal of calcium ions with calcium-quenching reagents such as sodium citrate, which allow for improved diffusion in the microbeads [21].
Investigators are currently examining different approaches to address the problem of an inadequate supply of oxygen to encapsulated islet transplants. In a recent study, the effect of a combination of growth-hormone-releasing-hormone agonist and a controlled oxygen supply on the function of a bioartificial macrochamber was examined. In this study, islets were encapsulated and maintained within alginate slab configuration adjacent to an oxygen-permeable membrane to create an immune barrier and allow for oxygenation of the islet graft. The minimally invasive implantable chamber was shown to normalize blood glucose in streptozotocin-induced diabetic rodents for up to 3 months after subcutaneous transplantation [42]. In another study, investigators showed that encapsulation of solid calcium peroxide within hydrophobic polydimethylsiloxane resulted in sustained oxygen generation that lasted for more than 6 weeks and was enough to prevent hypoxia-induced cell dysfunction and death in insulin-producing cells [43]. Another important factor that affects the function of encapsulated islets is the morphology of the microcapsules used for the encapsulation. Spherical microcapsules are necessary for long-term functionality; irregularities or imperfections in the microcapsules can cause an immune response and inefficiencies in the delivery of nutrients resulting in loss of islet functionality [44].
Transplantation Site
Based on the issue of adequate nutrient supply as discussed above, it is necessary to find a site where encapsulated islets are in close contact with the bloodstream. Unfortunately, this is difficult as the site should combine the capacity to bear a large graft volume with close proximity to blood vessels. Transplantation of encapsulated islets is most commonly performed intraperitoneally, as it offers the advantages of laparoscopic implantation or through injection, and allows ample room to implant numerous microcapsules [13,45]. However, there are several disadvantages to this site. In addition to the problem of avascular supply discussed earlier, another major disadvantage is that microcapsules implanted intraperitoneally are vulnerable to an immune response from intraperitoneal T cells and macrophages [27,46,47,48] and have less access to the vasculature. This results in an increased likelihood of fibrotic growth over encapsulated islets, a loss of graft functionality and a delay in insulin uptake into the blood circulation [49].
Consequently, alternative transplantation sites have been investigated, including the liver [50], kidney capsule [51], subcutaneously [52] and into an omentum pouch [2,34,53,54]. In the study conducted by Toso et al. [50], microcapsules were injected into the portal veins of rats; however, the results showed that immunosuppressants were necessary to prevent fibrotic overgrowth, and the risk of hepatic thrombosis makes this approach impractical. The studies by Dufrane et al. that investigated implant sites such as subcutaneous and the kidney capsule showed that encapsulated islets implanted in these two sites had less cellular overgrowth compared to encapsulated islets implanted intraperitoneally. Dufrane et al. [51] demonstrated the functionality of encapsulated islets implanted within the kidney capsule of primates; however, clinical application would be difficult, given the limited space within this site [55]. The attraction of the omentum pouch is that, like the kidney capsule, it offers a well-vascularized site for transplantation but has more space for microcapsules and is easier to access than the kidney [56]. In addition, microencapsulated islets transplanted in the omentum pouch are easily retrievable for posttransplant evaluation [2].
Summary and Conclusion
It is clear that the microencapsulated islet technology has enormous potential to achieve the ultimate goal of routinely performing islet transplantation in patients without the need for risky immunosuppressive drugs to prevent transplant rejection. The modern era of this technology began with the report by Lim and Sun [57 ]that a single implantation of microencapsulated islets into rats with streptozotocin-induced diabetes corrected the diabetic state for 2-3 weeks. In addition, the paper showed that the microencapsulated islets remained morphologically and functionally intact throughout long-term culture studies lasting over 15 weeks. Since that publication, interest in the technology has waxed and waned as various groups have obtained variable results with their microencapsulated islet constructs in preclinical studies sometimes performed with insufficient consideration of the critical factors required for optimal function of the islets. Thus, we have seen studies performed with islets microencapsulated in microcapsules without perm-selectivity, and studies performed with microcapsules fabricated without due consideration for the enhanced diffusion of nutrients and oxygen. The high oxygen requirements of islets need to be taken into consideration during all processes involved in the development of the technology. These processes include the islet isolation process as well as the microencapsulation technique itself, as encapsulated dead cells have no functional value. We have recently discussed the various factors that are necessary for the optimal functioning of encapsulated islets [2,11]. One of these limiting factors is the absence of high-throughput devices for the timely mass production of viable islets for studies in large animals and humans. Recent developments in cell microencapsulation described by our group have now provided the much-needed procedure to enhance the clinical application of the microencapsulated islet technology [34,35].
Although, as we have pointed out in this article, the microencapsulated islet technology as we presently know it has not been optimized, studies have since been initiated in humans, beginning with the first experiment performed by Soon-Shiong et al. [12] that reported insulin independence in a type 1 diabetic patient after encapsulated islet transplantation. In the experiment, encapsulated human islets were injected intraperitoneally into the diabetic patient with a functioning kidney graft, and insulin independence with tight glycemic control was demonstrated 9 months after the procedure. Since this report, other groups have performed studies with microencapsulated islets in human subjects and have obtained variable results [13,14,58]. When evaluating these studies, it is very important to consider if the critical factors such as the method of encapsulation including adequate perm-selectivity and mechanical strength of the microcapsules, the site of transplantation and the delivery of oxygen to the encapsulated islets were adequately addressed in the design of each study. An ongoing clinical trial with encapsulated neonatal pig islets in diabetic patients has shown some promise and is currently in phase II in New Zealand and Argentina [15]. One can only hope that with adequate optimization, the microencapsulated islet technology will someday offer a cure for type 1 diabetes.
Acknowledgements
The authors gratefully acknowledge generous financial support from the National Institutes of Health (grant No. R01DK080897) and the Vila Rosenfeld Estate, Greenville, N.C. for the studies on the bioartificial pancreas in Dr. Opara's (E.C.O.) laboratory.
